The General Practice Services Committee (GPSC) is implementing changes to incentive fees for family doctors starting April 1, 2020 that will streamline, clarify, and improve rule consistency across fees.
March 31 update: Updated fee guides posted on GPSC fees page.
GPSC is hosting a webinar for family physicians on Tuesday, March 24 at 6 p.m. to walk through the April 1 changes, any COVID-19 related fee changes that affect family physicians, and Pathways tools for COVID-19 care.
Note: If you've already registered for the webinar, please re-register as this is a new webinar account that allows more people to join the session.
Family physicians can continue to reach GPSC staff for billing support at gpsc.billing@doctorsofbc.ca.
Here are the top things to know about the incentive fee changes:
1. More fees are moving behind the portals
All GPSC fees billed by the Most Responsible Provider (MRP) are moving behind the 14070 and 14071 portals. Starting April 1, all fees for complex care, chronic disease management, prevention, mental health, and palliative care will be behind the 14070 and 14071 portals. Click here for fee codes moving behind the 14070/14071 portals.
Family physician MRPs and their locums must submit the appropriate portal code each year to access most GPSC fees.
Please note that submitting and meeting the requirements of portal code 14070 is also a requirement for receiving the GPSC Community Longitudinal Family Physician (CLFP) payment. Submitting 14070 signifies a family physician is providing full-service family practice services to their patients for the duration of the calendar year, and is confirming their doctor-patient relationship with existing patients through a standardized conversation or “compact”.
2. Some billing changes to support team-based care
Building on previous changes to support team-based care, the following enhancements have been made:
- Now billable on the same day: 14076 (FP Patient Telephone Management Fee) and 13005 (Advice about a Patient in Community Care Fee).
- Now billable on the same day: 14029 (Allied Care Provider Practice Code) and 14077 (Family Physician Conference with an Allied Care Provider and/or Physician Code).
Further details can be viewed here.
3. Revisions to the GPSC Preamble
Updates to the GPSC Preamble will ensure consistency of terms used across fee items and provide clarity to the interpretation of GPSC fee rules. The definitions of Allied Care Provider (ACP) “working within” the practice team vs “employed by” the practice have been clarified. Other clarifications include that “face to face” means “in person”. Detailed definitions of “most responsible provider” and “locum tenens” have also been created and should be reviewed. Click here for details.
4. New ICD-9 codes for mental health fees
To simplify billing, GPSC has updated the list of eligible diagnoses and ICD-9 codes for mental health planning and management fees. Make sure to use the revised ICD-9 codes. Click here to view the revised table of eligible ICD-9 codes.
5. GPSC Obstetrical delivery fees will now only be accessible to physicians registered in a maternity network and/or who’ve submitted the 14070/14071 portal codes
Obstetrical delivery fees 14004, 14005, 14008, 14009 will now be accessible only to family physicians who have submitted the portal codes and/or are part of a maternity network. Click here for details.
6. A new application process for physicians with consultative expertise to access billing codes 14021, 14022, 14023
There’s a new registration process for family physicians with consultative expertise working in health authority approved or supported programs who wish to access fees 14021, 14022 and 14023. Click here for more details including affected fee codes and a link to the application form.
7. For physicians on alternate payment and alternate funding models
There’s a new telephone management encounter code to be used if one of the two qualifying visits for chronic disease management is done by phone. Click here for fee codes.
Detailed Changes
1. More fees are moving behind the portals
All GPSC fees intended for the Most Responsible Provider (MRP), including complex care and chronic disease management fees, are moving behind the 14070 and 14071 portals. Family physicians and their locums must submit the appropriate portal code each year to access many fees including fees for complex care and chronic disease management.
- MRP family physicians submit portal code 14070.
- Locums providing coverage for MRP family physicians submit portal code 14071.
Submit the appropriate portal code as early as possible each year to access these fees, which transfer from GPSC to MSP on April 1st.
The following fees will be behind the 14070 and 14071 portals as of April 1, 2020:
- 14050, 14051, 14052, 14053 (Chronic Disease Management).
- 14066 (Prevention).
- 14033, 14075 (Complex Care).
- 14063 (Palliative Planning).
- 14043 (Mental Health Planning).
- 14044, 14045, 14046, 14047, 14048 (Mental Health Management).
As a reminder, the following fees are already accessed through the 14070/14071 portal codes:
- 14029 (Allied Care Provider Practice Code).
- 14075 (Complex Care Planning and Management Fee-Frailty).
- 14076 (FP Patient Telephone Management).
- 14077 (FP Conference with Allied Care Provider and/or Physician).
- 14078 (FP Email/Text/Telephone Medical Advice Relay).
2. Some billing changes to support team-based care
Building on previous changes to support team-based care, the following enhancements have been made:
- 14029 (Allied Care Provider Practice Code) and 14077 (Family Physician Conference with an Allied Care Provider and/or Physician Code) are now billable on same day.
Family physicians who delegate aspects of patient care to a college-certified allied care provider (ACP) often provide care to the same patient on the same day, billing for only one of the services as per previous billing requirements.
Effective April 1, 2020, family physicians who delegate one of the two required visits for chronic disease management care to a college-certified ACP working within their practice and bill 14029 will also be able to bill 14077 when a conferencing service is also provided by the family physician. A family physician who conferences with a college-certified ACP (or other eligible provider, including specialists) about a patient who has a chronic disease management visit with a college-certified ACP on the same day may bill both 14029 and 14077.
| New rule effective April 1, 2020: | Old rule: |
| Note (iii) for 14029 rule will state: “Not billable on the same calendar day as a visit or service fee by same physician for same patient, with the exception of 14077.” | Previously, the rule for 14029 stated: “Not billable when the patient has had a same day service provided and billed by the family physician.” |
- 14076 (FP Patient Telephone Management Fee) and 13005 (Advice about a Patient in Community Care Fee) are now billable on same day.
A family physician who provides advice with a patient in community care as required under 13005 and conducts a telephone visit (or delegates the telephone visit to a college-certified ACP employed by the practice) about the same patient on the same day may bill both 13005 and 14076.
| New rule effective April 1, 2020: | Old rule: |
| Note (vii) for 14076 will state: “Not payable on the same calendar day as a visit or service fee by same physician for same patient, with the exception of 14077, 14018, 14050, 14051, 14052, 14053, 13005.” | Previously, the rule for 14076 stated: “Not payable on the same calendar day as a visit or service fee by same physician for same patient, with the exception of 14077, 14018 14050, 14051, 14052, 14053, 14250, 14251, 14252, 14253.” |
3. Revisions to the GPSC Billing Guide Preamble
As of April 1, 2020, the GPSC Preamble will include updates that ensure consistency and provide clarity to the interpretation of GPSC fee rules.
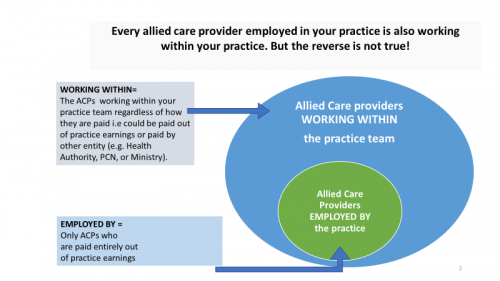
There are important differences in the rules around delegation of services depending on whether the Allied Care Provider is “employed by” a physician practice vs. “working within” a physician practice team.
Clarifications have been made to the definitions as laid out below:
Allied Care Provider “Employed by” a Physician Practice:
For the purposes of its incentives, GPSC defines Allied Care Providers (ACPs) “employed by” a physician practice as ACPs who are employed by a physician practice and paid out of practice earnings to work directly within the practice team, with no cost recovery either directly or indirectly from a third party (e.g. Health Authority, Division of Family Practice, Ministry of Health, etc.), unless otherwise specified.
Allied Care Provider “Working Within” a Physician Practice Team:
For the purpose of its incentives, GPSC defines Allied Care Providers (ACPs) “working within” a physician practice team as ACPs who work as part of an FP (family practice) practice’s team to support the ongoing care of its patients. The costs of an ACP “working within” the practice team may be paid either by the physician practice or by a third party (directly or indirectly). ACPs employed by a health authority are considered to be “working within” the practice team if they are assigned to work with an FP practice to support the longitudinal care of its patients. By contrast, ACPs not assigned to work with an FP practice and who provide episodic services to patients on a referral basis such as through specialized health authority programs or in stand-alone chronic disease clinics are not considered to be “working within” the physician practice team.
Some physicians find the diagram below helpful:
Additions
Several terms previously used in GPSC billing guides will now be added to the GPSC Preamble. The GPSC Preamble only applies to current GPSC fees and transferring GPSC fees. It does not apply to MSP fee listings.
Additional terms are added to the GPSC Preamble for the purposes of incentives.
| New term: | GPSC Preamble definition: |
| Care Plan |
The GPSC Preamble lists core elements that are required documentation in the patient chart |
|
Face-to-Face |
In-person |
| Locum Tenens | A physician with appropriate accreditation who substitutes on a temporary basis for another physician who is away from practice |
| Most Responsible Physician/Provider (MRP) | A physician who takes responsibility for directing and coordinating the ongoing care and management of a patient. This includes coordinating clinical services delegated to other providers, ensuring cross coverage when MRP is unavailable, and coordinating referrals to specialty care when needed |
| Patient Panel | The group of patients for which a family physician has assumed the role of MRP, and has confirmed their ongoing patient-physician relationship |
| Patient Self-Management | Decisions and behaviours that patients with chronic illness engage in that affect their health. Self-management support is the help given to patients with chronic conditions that enables them to manage their health on a day to day basis. There are a variety of publically available tools that FPs can provide to patients, to help build the patients’ skills and confidence to manage their chronic conditions |
| “Family Physician with Consultative Expertise” replaces “GP with specialty training” | GPSC defines a Family Physician with Consultative Expertise as: “A family physician who has consultative expertise and provides consultative services or support to colleagues through a health authority supported or approved program”. Examples of health authority supported programs include (but are not limited to) mental health, addictions, palliative, chronic pain, and emergency medicine. |
Revisions
To reflect the current language used in the field to describe physicians who specialize in family medicine, some terms used within the GPSC fees and Preamble will be revised as follows:
- “GP” to “FP.”
- “GP with specialty training” to “FP with consultative expertise.”
Additionally, the term “residential care” will change to “long-term care” in recognition of the Truth and Reconciliation process in Canada and with BC’s Indigenous peoples, and the importance of supporting the provision of patient-centered culturally safe care.
Changes to the language in the GPSC Preamble do not affect how family physicians bill GPSC fees.
| New language: | Old language: |
| FP | GP |
| FP with consultative expertise | GP with specialty training |
| Long-term care | Residential care |
4. Use updated ICD-9 codes for mental health fees
To simplify billing, GPSC reviewed and streamlined the list of eligible diagnoses and ICD-9 codes for mental health planning and management fees . The updated list of diagnoses and ICD-9 codes is available in the GPSC Mental Health Billing Guide.
For Mental Health fees 14043 (Mental Health Planning) , 14044, 5, 6, 7, 8 (Mental Health Management), be sure to use the updated ICD-9 codes, listed in the table below:
| Category | Diagnosis | ICD-9 |
| Anxiety Disorders | Anxiety Disorders | 300, 308, 50B |
| Bipolar and Related Disorders |
Bipolar |
296 |
|
Cyclothymia |
301.13 |
|
| Depressive Disorders | Depressive disorders | 311 |
| Dissociative Disorder | Dissociative Disorders | 300 |
| Eating Disorders | Eating Disorders | 307, 307.1 |
| Gender Dysphoria | Gender Dysphoria | 302 |
| Impulse Control Disorders | Impulse Control Disorders | 312 |
| Neurocognitive Disorders |
Delirium |
293 |
|
Dementia |
290, 331, 331.0, 331.2 |
|
| Neurodevelopmental disorders |
Attention Deficit Disorder |
314 |
|
Autism Spectrum Disorder |
299.0 |
|
|
Pervasive Developmental Disorder |
299.0 |
|
| Obsessive-Compulsive & Related Disorders |
Obsessive-Compulsive Disorder |
300 |
|
Body Dysmorphic Disorder |
300.7 |
|
| Schizophrenia and other Psychotic Disorders | Schizophrenia and other Psychotic Disorders | 293, 295, 297, 298 |
| Sexual Dysfunction | Sexual Dysfunction | 302 |
| Sleep Disorders |
Sleep wake disorders: Insomnia/ hypersomnolence/ narcolepsy |
307.4, 347 |
|
Parasomnias |
307.4 |
|
|
Breathing-Related Sleep Disorders |
780.5 |
|
| Somatic Symptom & Related Disorders |
Factitious Disorder |
300, 312 |
|
Pain Disorder with Affective Symptoms |
338 |
|
|
Somatic Symptom Disorder |
300.8 |
|
|
Conversion Disorder |
300.1 |
|
| Substance Use Disorders |
Substance Use Disorder: Alcohol |
303 |
|
Substance Use Disorder: Drugs |
304 |
|
| Trauma and stressor related disorders |
Adjustment Disorders |
309 |
|
Post-Traumatic Stress Disorder |
309 |
5. Maternity codes 14004, 14005, 14008, 14009 are now accessible only to physicians registered in a maternity network and/or who’ve submitted the 14070/14071 portal codes
Obstetrical delivery fees will now be accessible only to family physicians who have submitted the portal codes and/or are part of a maternity network.
- 14004 (Obstetric Delivery Incentive for Family Physicians – associated with vaginal delivery and postnatal care).
- 14005 (Obstetric Delivery Incentive for Family Physicians – associated with management of labour and transfer for delivery to a higher level of care facility).
- 14008 (Obstetric Delivery Incentive for Family Physicians – associated with postnatal care after elective caesarean-section).
- 14009 (Obstetric Delivery Incentive for Family Physicians – associated with attendance at delivery and postnatal care associated with emergency caesarean section).
6. New application process for family physicians with consultative expertise to access billing codes 14021, 2, 3
There will be a new annual application process for GPSC fees that support family physicians with consultative expertise (previously called “GPs with Specialty Training”) who work in a health authority-approved or supported program.
- 14021 FP with Consultative Expertise Telephone/Video Advice – Response within 2 hours.
- 14022 FP with Consultative Expertise Telephone/Video Advice – Response within 1 week.
- 14023 FP with Consultative Expertise – Patient Telephone/Video Management/Follow-Up.
7. For family physicians on alternate payment/ funding models: New telephone management encounter code: 14276
GPSC is introducing a new telephone management encounter code (14276) for family physicians on alternate payment who use the designated chronic disease management (CDM) fees:
- 14250, 14251, 14252, 14253 (Chronic disease management for physicians on alternate payment who bill encounter record visits).
The new encounter code helps ensure that eligible family physicians on alternate payment/funding models can demonstrate their provision of guideline-informed care over a 12-month period. Physicians on alternate payment/funding models may demonstrate guideline-informed care by providing at least two visits with eligible patients, whereby one of the two visits can be an in-person visit with an ACP or a Group Medical or a Telehealth visit, or a telephone visit which is now billable under 14276.
Physicians may also demonstrate guideline-informed care by providing an office visit, group medical visit, or by submitting 14029 after delegating a visit to a college-certified allied care provider working within the family physician practice.